Updated:
June 9, 2026
Commercial Surrogacy
We oppose commercial surrogacy, which treats children as commodities and exploits vulnerable women.
Psalm 100:3: “…it is [God] who made us, and we are his…”
The process
Commercial surrogacy involves contracting with a woman called the “surrogate mother” or “gestational carrier” to carry and birth a baby for another person or couple. Although commercial surrogacy is not legal or regulated by the Minnesota government, the industry practices in Minnesota.
The egg and sperm may be provided by the couple who will parent the child. The egg and/or sperm could also be purchased from the egg and sperm bank industry (inaccurately called “donor” egg and sperm,) which provides anyone with financial resources the gametes desired.
The person or couple who will raise the child, the “Intended Parent(s,)” IP(s), pay for the gametes desired based on the characteristics of the gametes and the individual selling, with factors such as height, eye color, intelligence, and athleticism in consideration. The IPs also pay for the fertilization process by an IVF clinic.
Gametic material of egg and sperm are fertilized in a lab (see MFC statement on IVF,) and one of the embryos is selected for placement into the surrogate mother for the pregnancy. Preimplantation genetic testing is often conducted to ensure that a selected embryo has the physical traits desired by the IPs and does not show chromosomal abnormalities.
Unlike adoption, there are generally no requirements for IP(s) to undergo background checks, interviews, and home studies. Financial resources are the only qualification. If the pregnancy goes according to contractual obligations and the baby is born, the IPs pay the surrogate for womb rent and labor, assuming legal custody of the child and removing the child from the child’s only known mother – the surrogate.
Genetic surrogacy occurs when the surrogate mother also provides the egg for the baby. This practice is generally not sanctioned as it is legally deemed more closely related to baby selling than commercial surrogacy.
Surrogacy involves the intentional separation of a child from his or her birth mother for placement with either related or unrelated adult(s).
Minnesota Family Council opposes the legalization of commercial surrogacy.
In Minnesota, commercial surrogacy is extra-legal. Commercial surrogacy contracts are drawn up and fulfilled in Minnesota, but they do not have the protection of Minnesota state law to ensure that contracts must be fulfilled. Although a surrogate mother may essentially sign away her medical rights to people paying her to carry a baby, the legal authority to require her to follow the contract is lacking.
For this reason, various parties in the commercial surrogacy industry such as the surrogacy agencies or the attorneys representing the IPs ask Minnesota legislators to “regulate” the industry. They are seeking legal backing to enforce the contracts, securing profit.
As explained previously, commercial surrogacy intentionally and necessarily separates a child from his or her birth mother. State statute must protect the best interests of the child, which under most circumstances is to keep a child with his or her biological parent(s).
Commercial surrogacy is a process by which children are created to be separated from their mothers, whereas adoption rescues a child from parental loss after birth. Children are not conceived to be placed into the adoption system, but children are conceived in commercial surrogacy to be, in effect, sold.
On begetting babies rather than making babies
We affirm the dignity and value of every human life, regardless of conception status.
We hold that children are begotten, not made. A unique life begins when egg and sperm fertilize, and each embryo is a distinct human. Each human is a subject of rights, not the least of which is the right to life at the embryonic stage.
We affirm the reality of human biological design that sex and procreation are not divided; the design of the male and female body attest to the reality that they must come together for procreation. The fact that procreation does not always result from the act does not negate this reality.
On navigating infertility
We know that couples struggling with infertility face great heartbreak, pain, and difficult decisions as they navigate loss from infertility. We recognize the lack of healthcare that women and couples have received as most fertility clinicians bypass the health issues patients are facing, focusing only on the product of a healthy baby. Even if a baby is born, the underlying medical condition of the mother or father remains, unless treated.
Many couples who struggle with infertility have either one or multiple underlying health conditions which should be addressed through medical care. When these underlying conditions are addressed, the couple can increase their likelihood of achieving pregnancy. While an underlying medical condition is not always the cause of infertility, for many couples, this is the cause. We encourage couples to get a good diagnosis of their personal factors for infertility and seek medical care for those factors.
We support public policy efforts to advance family preservation whenever possible, to protect children, and to promote restoration of health of the body, which can also repair fertility. We support technologies that seek to restore reproductive health rather than technological efforts which intentionally bypass the health of the body. We advise couples considering technological efforts which intentionally bypass the body to exercise caution.
On third-party conception
We do not support third party methods of conception such as gametes for purchase (commonly called “donor” egg or sperm) which bring a third party into the conception and birthing of a child. To sell one’s gametes, a person sells half of his or her offspring’s genetic formation, with not insignificant risks to personal health. By using gametes of a third party in producing a child, the adult(s) seeking a child create to separate the child from a parent.
On standard practices of the industry
We oppose the standard practices of the assisted reproductive technology industry, practices which take more lives than they help to produce. Since 1990, preimplantation genetic testing of embryos has become a standard practice. This process involves extracting nuclei from either eggs or embryos for the purpose of testing for mutations. The American Society for Reproductive Medicine’s Fertility and Sterility Journal explains that providers “generally apply clinical guidelines to determine when PGT-M (preimplantation genetic testing) should be offered.” PGT-M is especially promoted if either of the parents has a history of chromosomal abnormality.
In an updated 2023 report, the ASRM acknowledges that preimplantation genetic testing can be problematic. The express purpose of genetic testing of either embryos or gametes is to determine the healthiest embryos with optimal genes, or to determine whether a person’s gametic material carries chromosomal abnormalities.
More recent developments by companies like Orchid conduct preimplantation genetic screening of the whole genome to analyze the embryo’s full genetic makeup. Orchid and similar companies provide whole genome analysis not just to prevent giving birth to a child with chromosomal abnormalities, but to choose an embryo which fits the characteristics desired by the parent(s). This is industrialized production of children.
Process of IVF
In vitro fertilization (IVF) is the process by which egg and sperm are fertilized outside the womb in a fertility laboratory. Although multiple procedures fall under the assisted reproduction technology (ART) industry, IVF and the ART cycles to achieve an embryo for implantation are some of the most common technologies.
For a couple trying to use their own egg and sperm to produce a child, an ART cycle consists of hormonal treatment of the woman to induce maturation and release of multiple eggs. A natural cycle usually results in one released egg per cycle, if the woman is healthy. The eggs are manually extracted from the follicles and fertilization is attempted by either placing the egg in a petri dish with sperm or by injection of sperm into the egg, called ICSI (Intracytoplasmic Sperm Injection.) Given the high cost and involvement of the process, labs usually create multiple embryos, if possible.
Any embryos created are then monitored for healthy development. After a few days, generally one embryo is chosen for implantation into the woman’s uterus, and the woman is given hormonal treatment for her uterus to receive the embryo. Additional embryos are stored in cryopreservation facilities (freezers,) “donated” for research (with subsequent destruction after 14 days,) or flushed away.
We affirm the inherent dignity and value of every human life, regardless of conception status. Although many children in recent decades have been born from IVF, most embryonic lives created through assisted reproductive technology (ART) do not survive, by intention of the fertility industry. The 2021 Assisted Reproductive Technology (ART) data from the Centers for Disease Control reported that 413,776 ART cycles resulted in 97,128 live-born infants in that year. Some of those cycles were conducted for freezing eggs only. Given the multiple embryos created in an ART cycle, there could have been as many as 4 million embryos created in 2021. With that estimate, 1 in 50 embryonic lives were born of the lives created by the industry.
FAQs
Should we consider embryo adoption?
Although the Assisted Reproduction industry in the United States lacks regulation, estimates have been made on the number of embryonic lives in cryopreservation facilities. The Johns Hopkins Bloomberg School of Public Health estimates, “There are over a million and a half embryos currently frozen across the U.S.” Married couples may be considering whether they are called to adopt a frozen embryonic life.
We first encourage couples to see any adoption not as a response to infertility but as a unique calling to welcome a child into a loving home. While we support couples’ efforts to rescue children from abandonment, there are some things to consider before adopting an embryo:
- This embryo will be placed into an unrelated woman’s womb. The woman’s body is not prepared to receive the embryo as it would be under natural pregnancy conditions, so her body must be treated to not reject the embryo. This lack of biological relationship creates stress on embryonic life.
- Seeking to give embryonic babies a chance at life is a beautiful goal. We also encourage married couples to prayerfully consider children who have been born and are waiting for a home in adoption agencies or foster care placement.
Don’t you understand that the country is facing an unprecedented fertility crisis? What other options exist for couples seeking to have children?
Yes, the Centers for Disease Control report that in the United States, lowering birth rates have been the trend since the early 2000s. Various factors contribute to these lowered rates, and one significant factor is impaired fertility. Underlying many cases of infertility are various diseases which should receive medical treatment. When couples struggle with infertility and seek care, many providers prescribe IVF exclusively as the solution.
When couples struggle with infertility and seek care, many providers prescribe IVF exclusively without providing care to the patients. IVF bypasses the body to secure the desired product of a child, but it does not heal the body. Reports estimate that IVF accounts for 99% of all assisted reproductive technology treatments. We encourage couples to seek treatment (Restorative Reproductive Medicine) which seeks to heal underlying diseases which impair reproductive function and in turn, often restore fertility.
Aren’t children happy in any home where the parent or caring adults love them?
It is a natural and good desire of a married man and woman to have children.
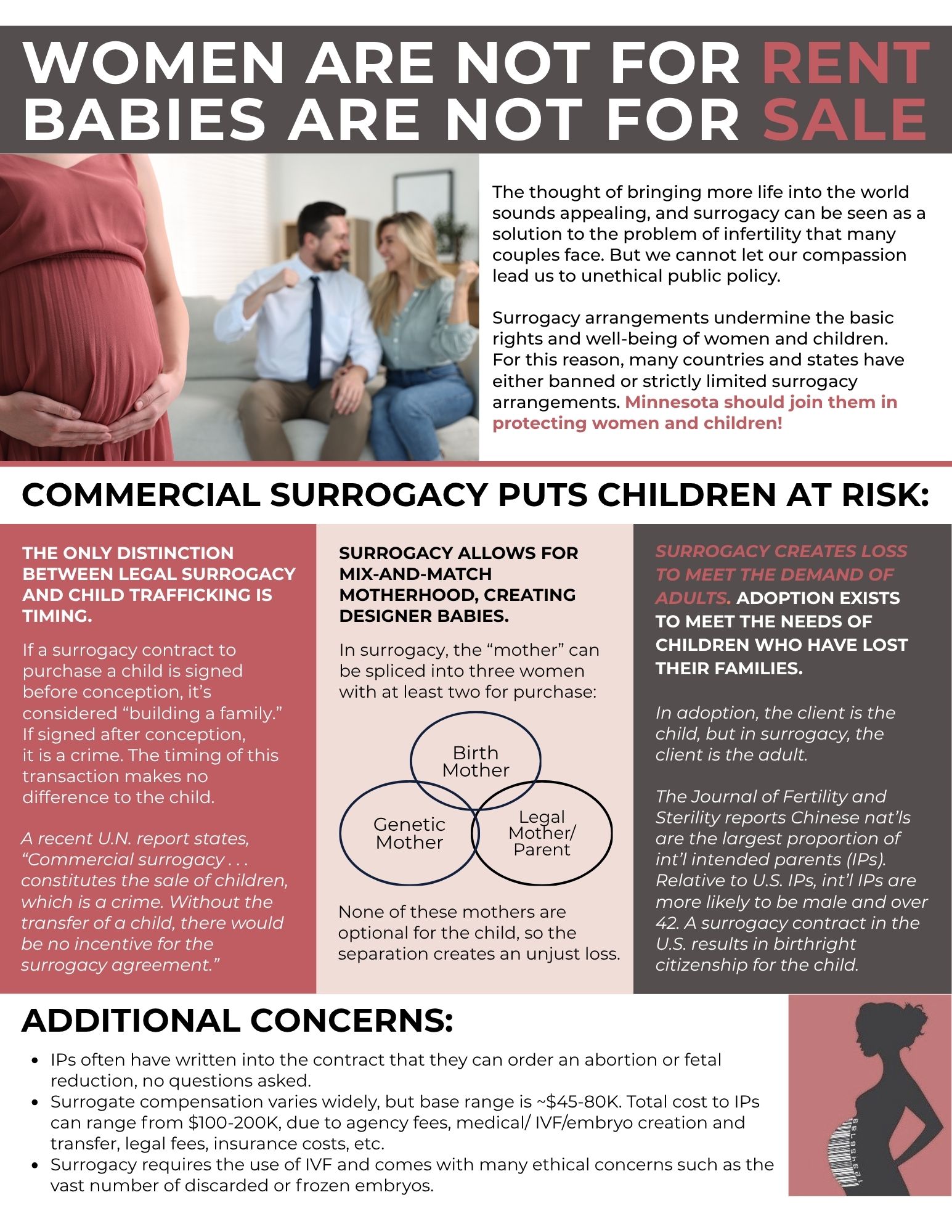
From a moral and public policy position, any technological effort to have a child must not involve the creation and sacrifice of other children, the siblings. In addition, by design, surrogacy is mix and match motherhood, in which three women can serve one part of motherhood, or one woman serves two parts: birth mother, genetic mother, and social/legal mother. In the case of surrogacy, there may also be no mother intended for the child.
Parent loss is not an unintended aspect of surrogacy – it is a part of the design of the process. Surrogacy intentionally separates a child from at least one of his or her parent(s). Creating babies with intentional parent loss is not a moral position.